
Gut Bacteria May Link Maternal, Child Weight
/
Overweight mothers tend to have overweight children, but the link is not entirely genetic. A new study suggests that the gut microbiome may play an important role.
Read MoreOverweight mothers tend to have overweight children, but the link is not entirely genetic. A new study suggests that the gut microbiome may play an important role.
Read MoreA study appearing in Annals of Internal Medicine has put a serious dent into the theory, referred to as the obesity paradox, that moderate increases in body fat are protective. For the video version, click here.
Read MoreA study appearing in the journal Pediatrics has identified four "BMI Trajectories" that kids in the UK seem to follow. But how do these trajectories affect their psychosocial development? For the video version, click here.
Read MoreTuna, shark, king mackerel, tilefish, swordfish. If you’ve ever been pregnant, or known someone who has been pregnant, this list of seemingly random aquatic vertebrates is all too familiar to you. It’s the “avoid while pregnant” list of seafoods, and it’s just one of the confusing set of messages surrounding pregnancy and fish consumption.
(For the video version of this post, click here).
Because aren’t we supposed to be eating more fish? Fish are the main dietary source for omega-3 fatty acids, which can cross the placenta, and may promote healthy brain development. Of course, some of these fish contain mercury which, as Jeremy Piven taught us all, may be detrimental to cognitive development.

These contradictory facts led the US FDA, in 2014, to recommend that pregnant women consume more fish, but not more than 3 times a week. You have to love the government sometimes.
A study appearing in JAMA pediatrics is making some waves with its claim that high levels of fish consumption, more than 3 times per week during pregnancy, is associated with more rapid neonatal growth as well as higher BMIs throughout a child’s young life. Now, contrary to what your mother-in-law has been telling you, more rapid infant growth is not necessarily a good thing, as rapid infant growth is associated with overweight and obesity in childhood and adulthood.
But fish as the culprit here? That strikes me as a bit odd. Indeed, prior studies of antenatal fish consumption have shown beneficial or null effects on childhood weight gain. What is going on here?
The authors combined data from 15 pregnancy cohort studies across Europe and the US, leading to a final dataset including over 25,000 individuals. This is the studies greatest strength, but also its Achilles heel, as we’ll see in a moment.
But first the basic results. Fish consumption was based on a food frequency questionnaire, a survey instrument that I, and others, have a lot of concerns about. Women who reported eating less than or equal to 3 servings of fish a week had no increased risk of rapid infant growth or overweight kids. But among those eating more than 3 servings, there was around a 22% increased risk of rapid growth from birth to 2 and overweight at age 6.

These effects were pretty small, and, more importantly, ephemeral. The authors looked not only at the percentage of obese and overweight children, but the raw differences in weight. At 6 years, though the percent of overweight and obese kids was statistically higher, there was no significant weight difference between children of mothers who ate a lot of fish and those who didn’t. When statistics are weird like this, it usually suggests that the effect isn’t very robust.
In fact, this line from the stats section caught my eye, take a look:

That means the authors used numbers predicted by a statistical model to get the weight of the children rather than the actual weight of the children. I asked the study’s lead author, Dr. Leda Chatzi, about this unusual approach and she wrote “Not all cohorts had available data on child measurement at the specific time points of interest… in an effort to increase sample size and…power in our analyses, we…estimated predicted values of weight and height”.
So we have a statistical model that contains as a covariate, another statistical model. This compounds error into the final estimate, and in a study like this, where the effect size is razor thin, that can easily bias you into the realm of significance.
And, at this point it probably goes without saying, but studies looking at diet are always confounded. Always. While the authors adjusted for some things like maternal age, education, smoking, BMI and birth weight, there was no adjustment for things like socio-economic status, sunlight exposure, diabetes, race, or other dietary intake.
What have we learned? Certainly not, as the authors suggest, that

That they wrote this in a study with no measurement of said pollutants is what we call a reach.
Look, you probably don’t want to be eating fish with high levels of mercury when you are pregnant. But if my patients were choosing between a nice bit of salmon and a cheeseburger, well, this study doesn’t exactly tip the scales.
For the video version of this post, click here. Weight loss is something of a holy grail for pharmaceutical companies. A large and, frankly, growing market exists not only in the US but around the world, and is only getting bigger. The list of drugs that have tried, and failed, to crack this market is ever-growing.
Weve recently seen a slew of news reports about the SCALE study touting the injectable medication liraglutide, now being marketed by Novo Nordisk as Saxenda.
The mainstream news outlets have done their job getting the details of this trial out there,

but when your patients ask you about liraglutide, you might want a little more detail than what you get from CNN. So, this week, were taking a second look at the SCALE study.

Lets start at the beginning.

Liraglutide is a glucagon-like-peptide 1 analogue, and, as a peptide, can only be given by injection. GLP-1 is in the incretin family - it increases insulin and insulin sensitivity, delays gastric emptying, and promotes feelings of satiety. As such, liraglutide was originally tested in, and approved for use in, individuals with type 2 diabetes. That weight loss was a side-effect was I think a happy accident for Novo Nordisk.
The trial, as its presented, was pretty straight-forward. We have roughly 3700 non-diabetic patients with a BMI greater than 30 or 27 if they had a relevant comorbidity randomized to liraglutide or placebo and followed for 56 weeks.

They also got lifestyle intervention. The endpoint was change in weight, and it was pretty clear that the liraglutide group lost more than the placebo group - around 8 kilograms versus 3 kilograms.

The news outlets have, appropriately, pointed out that for 5 kilograms of weight over a year, the $1000 a month price tag might not be reasonable, but we can dig a bit deeper than that.
Lets talk study design. First of all, check out this sentence regarding statistical power.

This study was designed with a whopping 99% power to detect a positive outcome. Actually, by my calculation, it was around 99.99% power. If Novo Nordisk was going for a more traditional 90% power, they would only have had to recruit around 150 individuals. In other words, they were betting BIG on this drug. Whether it paid off is still up for grabs.
Heres another point worth noting - statistical analysis and editorial assistance for the manuscript were provided by Novo Nordisk. Given that most of the endpoints were pre-specified, they didnt have too much flexibility to massage the data, but I think it would be informative to consider what doesnt appear in the manuscript.
Take a look at Figure 1 here.
This is the important figure - weight-loss in the two comparison groups. How would you interpret the error bars? If they are standard deviations, the graph would suggest that weight loss was remarkably consistent in the liraglutide group. But those error bars arent standard deviations, they are standard errors - a subtle difference, but one with a big impact. Heres what the graph would look like with standard deviations.
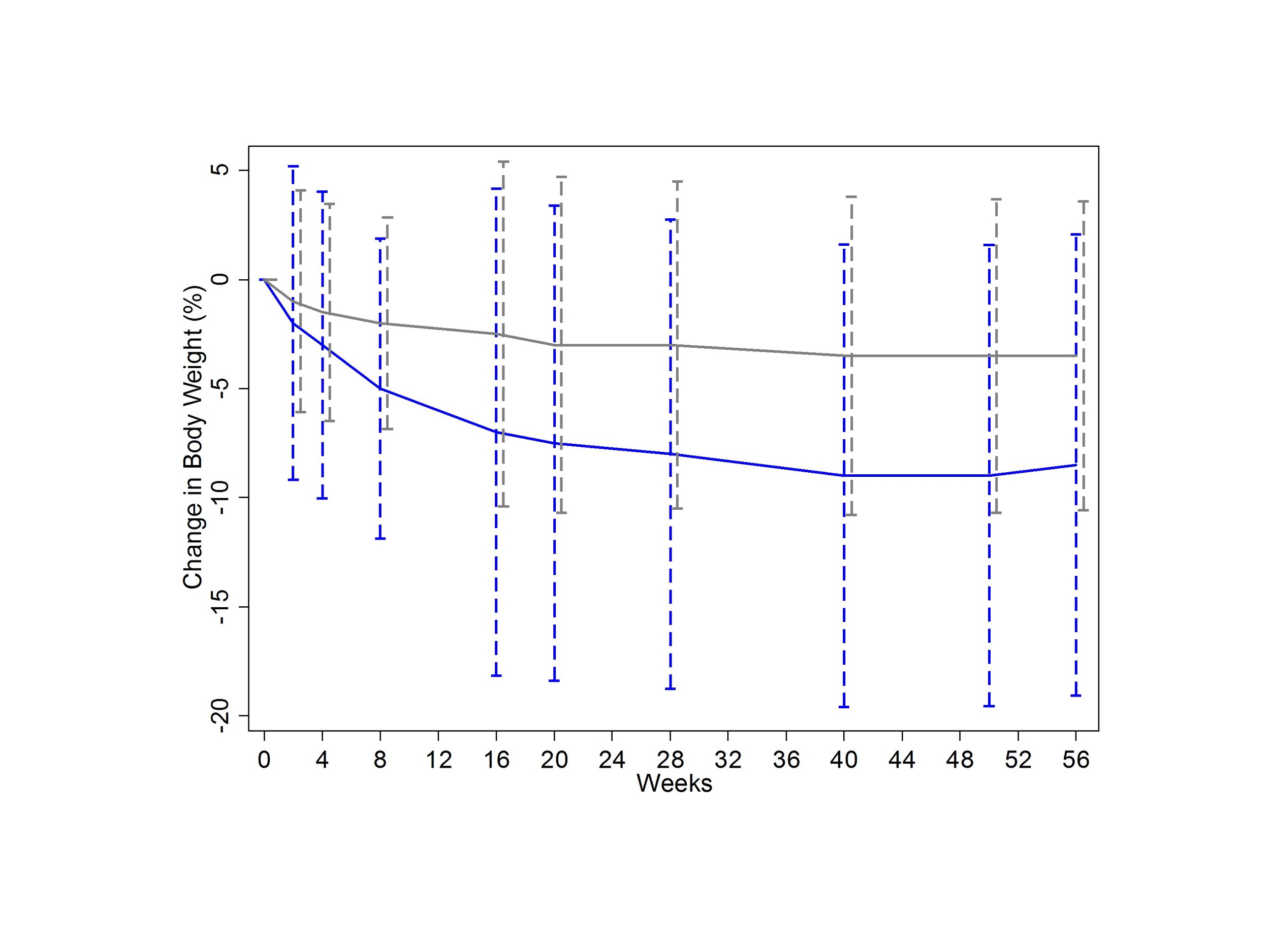
This would help to drive home the fact that, although the drug seems to work, your mileage may vary.
Theres also no discussion of how well blinding worked. Did people who got placebo know they were getting placebo? Reading between the lines, it seems pretty clear that they did. 20% of the placebo group withdrew their consent for the study, only 10% of the liraglutide group did.
They could probably figure it out because the side-effects of liraglutide were so clear. 25% of liraglutide patients had nausea in the first four weeks, as this graph shows.

One other analysis I would have liked to see? Adjust the outcome for the side-effect symptomatology. In other words, do people lose weight because they feel sick, or is that just an unlucky effect that occurs in some. It wouldnt invalidate the results, certainly, but it would certainly help us counsel patients.
Now, this trial was conducted in 27 countries at 191 different sites. The company would state that they did this to increase generalizability. There are some more cynical reasons to do this though. Number one, its a lot cheaper to do these studies outside of the US. But research oversight can also be a bit more lax.. in other countries. Despite my searching, I was unable to turn up how many of these patients came from the US. In a study where blinding was likely incomplete, it would be very interesting to see if certain recruitment sites had spuriously high effect sizes.
Now let me be clear, Im not saying anything untoward happened here, only that the data would be nice to have.
As for the main issue you see in the press? That the drug is too expensive for its modest efficacy? Lets not throw the baby out with the bathwater. One interesting secondary outcome was the rate of new diabetes diagnoses - low overall, but 7-fold higher in the placebo group.
One unfortunate, though unsurprising, finding was that the weight comes back when you stop using the drug, as evidenced from an extension trial in the liraglutide arm. So this might be a life-long drug. Good for Novo Nordisk, but bad for patients.
After a second look, where are we left with liraglutide? Well, the drug causes weight loss, in most people. It causes side-effects, in a lot of people. It may prevent diabetes. It costs a lot. The rate of uptake is going to be heavily dependent on calculations done by the insurance companies. If the co-morbid conditions ameliorated or prevented by the weight loss will save money, well see it get used. But its not a permanent fix. Theres an elephant in the room that isnt mentioned in the manuscript, and in few of the news articles I read. Its called bariatric surgery, a one-time procedure which may have more efficacy than a lifetime of liraglutide. And though that wasnt the comparator in this trial, it may be the comparator in our patients heads.
Thats the skinny on liraglutide. Ill see you next time we need to take a second look.




