
It's Time for a National Coronavirus Thermostat
/Clear mitigation plans, established in advance, are critical for the next phase of the pandemic.
As COVID restrictions start to be lifted across the country, and as the harsh New England Winter starts to give way to a harsh New England Spring, my thoughts turn to my thermostat.
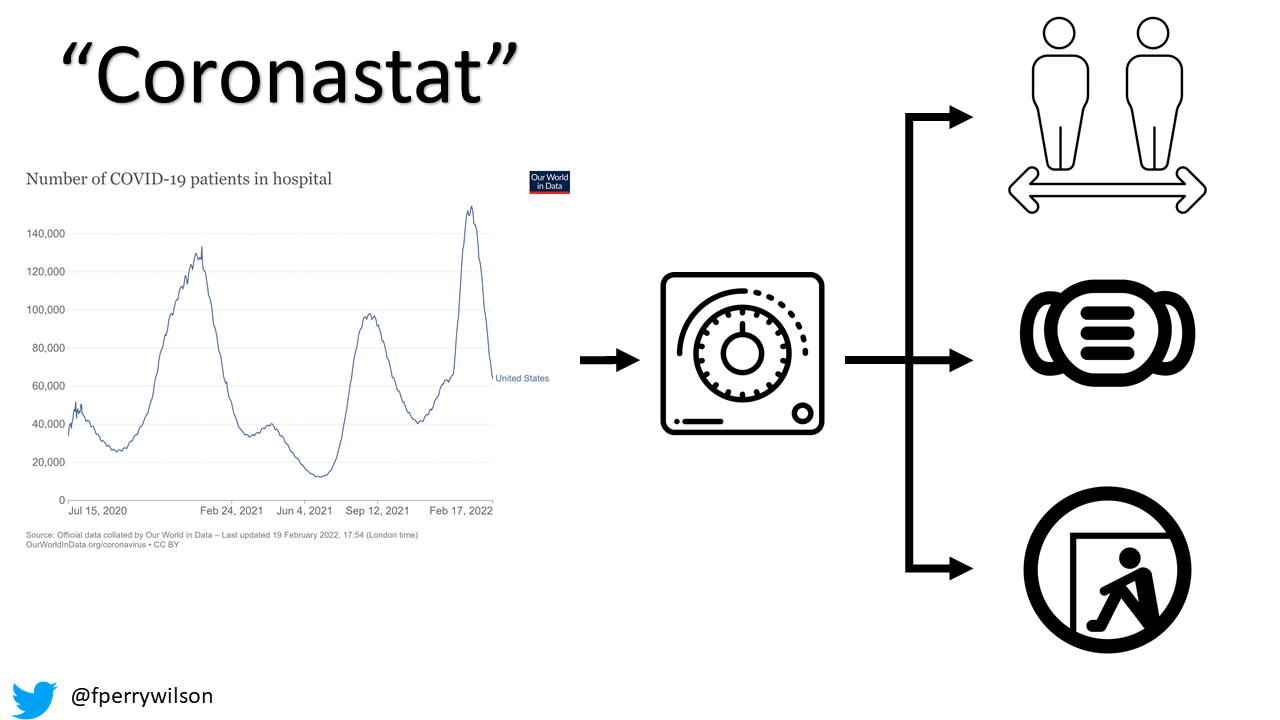
Yes, I think the humble thermostat can teach us a lot about public health in the COVID pandemic. In fact, I think it’s time we have a real, national COVID thermostat – a corona-stat - that we can look to to dictate mitigation efforts as the virus, increasingly endemic, ebbs and flows.
Just as a thermostat senses the ambient temperature and flips a switch to turn on the air conditioner, so to can we measure the burden of COVID in the community and engage in appropriate mitigation efforts.
Isn’t that what we’re doing already?
Hardly.
You know what my favorite thing about my thermostat is? That I know when it will turn on. I set a temperature – and when that temperature is hit – the air conditioner starts running. I do not have to react to the temperature change, running over to switch on the motor myself. It just happens – transparently – predictably. Imagine if we had that kind of guidance for COVID.
How would a corona-stat work? Well, thermostats have to sense the temperature. That’s easy. What metric should drive our Corona-stat?
Case rates is an obvious choice since they are blaring across TV screens all the time.
But that said, the relationship between cases and hospitalization depends on the virulence of the variant we’re talking about, how well it can avoid prior immunity, and how much of the population is immune. So case rates really aren’t the right input to our corona-stat; the meaning of a case now and a case 3 months from now may not be the same.
Hospitalization rates seem a more reasonable input choice, though I’m sure there would be debate here. Still, hospitalization is concrete. And clearly, hospitals filling up has public health impact that extends to the uninfected as well. So, for the sake of argument, let’s have hospitalization rate be the input.
We can have multiple outputs to the corona-stat. A threshold can trigger distancing requirements in public, a threshold could trigger indoor masking, a threshold could even trigger shelter in place orders.
The important thing is that we would set these thresholds before we reach them, like setting a thermostat. We avoid the issue of people feeling like they are at the whims of a fickle system.
There’s more to learn from thermostats though, for thermostats are not as simple as they seem.
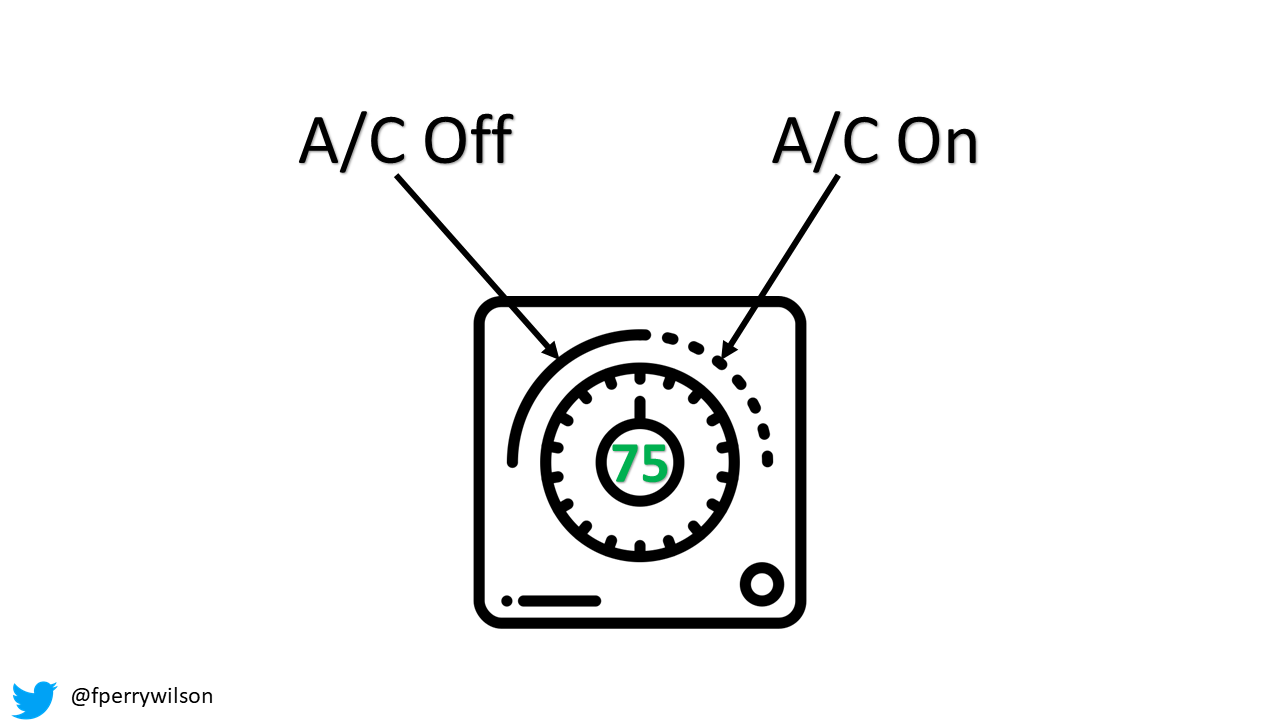
Take a thermostat that controls your air conditioning system. You specify a temperature you want – if you’re me 68 degrees – if you are my wife, like 75 degrees. Let’s compromise and say 75 degrees.
A simple thermostat would switch the AC on when the temperature went above 75 and turn it off when the temperature went below 75.
But this would actually be quite annoying in practice. It would be switching on and off constantly, as minor perturbations around that 75 degree mark flip the switch back and forth.
It is for that reason that modern thermostats have hysteresis – and it’s something our COVID mitigation policy needs as well.
Hysteresis is the dependence of the state of a system on its history. In thermostats, hysteresis means that the temperature where a thermostat switches from off to on may be different than the temperature when it switches from on to off.
So, if we’re targeting 75 degrees, we might switch on at 76 and off at 74. That buffer helps prevent cycling that would put wear and tear on the thermostat engine.
So it is with public health mandates for our COVID thermostat. You want your intervention – say indoor masking – not to switch on and off all the time – the public will get frustrated and potentially confused.
You need to build a buffer into the system. If indoor masking is “off”, perhaps rising above 50,000 hospitalizations triggers masks to be on again. If masking is “on”, you may need to fall below 25,000 to take them off. These numbers are just examples – the better way to do this is probably with local hospitalization rates.

You could even get fancier and have the coronastat behave differently when hospitalizations are rising versus falling. It might be better to start masking at a lower level when hospitalizations are on the upswing, and to take them off at a higher level when hospitalizations are decreasing – riding the wave of the virus so to speak.
The important thing is that you have clear guidance set in advance. Not only does this allow for proper planning, it will increase the rate at which individuals follow the guidelines. Because they are prepared.
Of course, thermostats are designed to maintain a constant temperature – a homeostasis. Does our Coronastat model mean our GOAL is to have a certain number of hospitalizations? That if we fall below that we are trying to push the numbers back up?
Of course not – the Coronastat is really just half of a thermostat – it is the A/C without the heating. It tries to keep hospitalizations below a given level, and to allow life to return to normal as much as possible provided we stay below that level. If hospitalizations drop to zero, that’s all good.
It’s tempting to think that we’ll be back to normal soon. Cases are falling. Hospitalizations are falling. Immunity is widespread. We may set the coronastat and never have it turn on. Wouldn’t that be wonderful. But we’ve been burned before. We may not know what tomorrow may bring in this pandemic, but clear, transparent contingency planning will ensure that tomorrow doesn’t surprise us.
A version of this commentary first appeared on Medscape.com.