
Are Kids COVID's Secret Weapon?
/High viral loads with minimal symptoms may be a recipe for disaster.
This week, one of the headline-generatingist COVID studies coming out in a while, appearing in the Journal of Pediatrics.
You’ve probably seen this one in the news. USA Today suggested that healthy kids may be more contagious than sick adults. Kaiser health news gave it a similar treatment.
And Fox news gives us this, for example:
The message from these headlines is pretty clear – but they all contain an error. That error… will become clear by the end of this commentary.
Ok let’s walk through the study because there are actually quite a few worthy take-home points here.
Researchers from MGH recruited kids who presented to the hospital or urgent care clinic with COVID-like symptoms or high-risk contacts – 192 in total making this one of the biggest pediatric cohorts to date. But only 49 of those kids were COVID-positive. Another 18 had the multisystem inflammatory syndrome that we are beginning to recognize as a post-covid complication in kids. The rest had other infections that give you upper respiratory symptoms.
First key takeaway – it was pretty hard to distinguish the acute COVID-infected kids from kids with other infections based on symptoms alone.

Anosmia was more common in COVID, but only 20% of the COVID-positive kids had that symptom. Fever was present in about half of kids regardless – that’s probably why they were in urgent care after all. Reading this gave me some real heartburn about what to do when cold and flu season ramp up – there are going to be a lot of kids who seem like they have COVID even if they don’t have COVID. And without ubiquitous testing, we won’t be able to tell the difference.
But the crux of this study, the thing that generated all those headlines, was a quantitative analysis of viral RNA in infected kids nasopharyngeal passages.
We’ll blow this figure up full screen because I really want to focus in here.
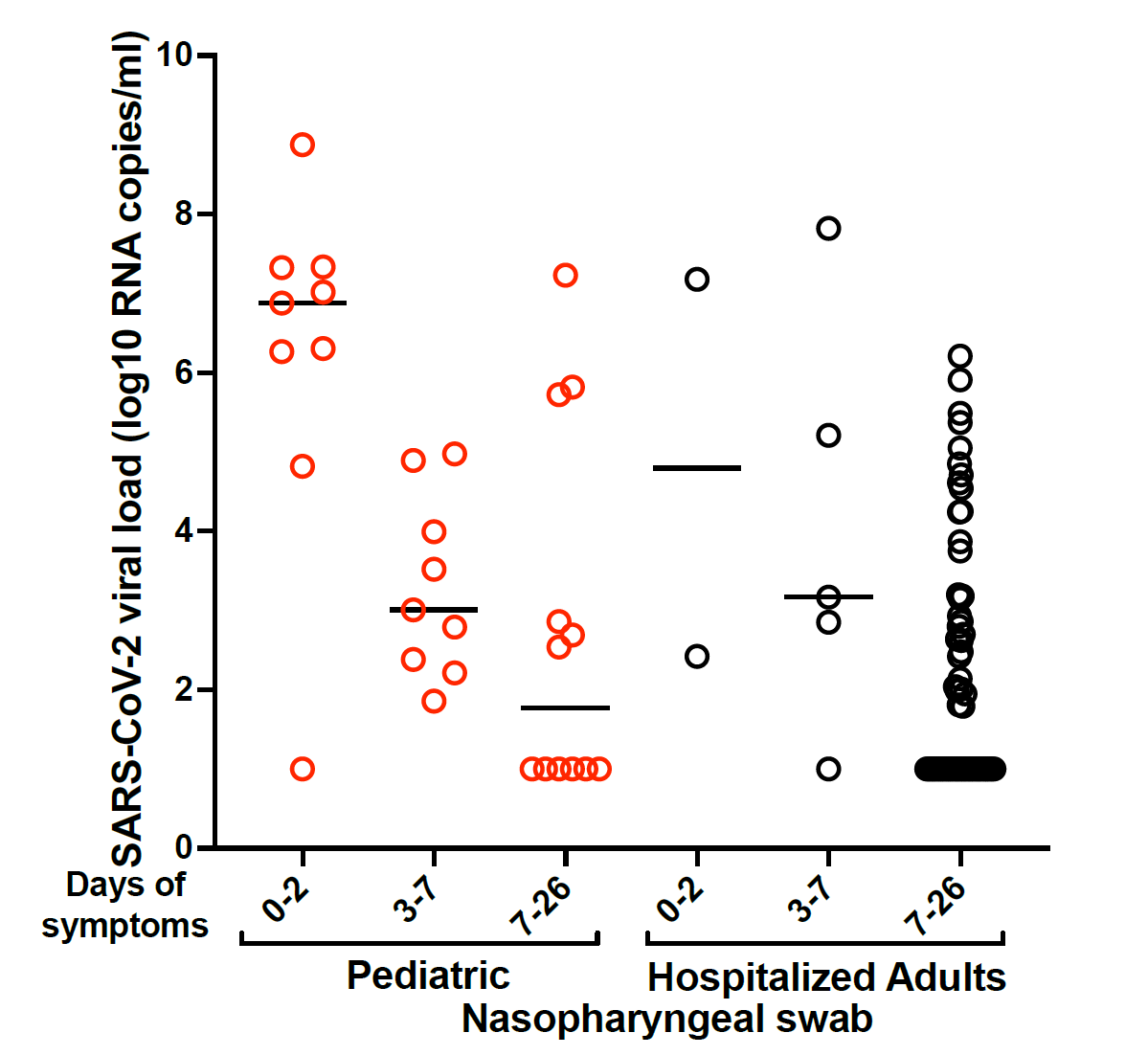
OK what you see here is how much viral RNA was present in the nasal swab as compared to a “housekeeping” gene that is expressed at a constant level – this helps account for differences in sample technique and collection volumes. Those circles way at the bottom – 1 on the y-axis, are the undetectable viral loads. But note that the y-axis is on the log scale – every point higher is a 10-fold increase in viral RNA. Kids, in red, were compared to severely ill adults – and you can see quite clearly that, at least early in the disease, some are shedding 10-, 100-, 1000- fold more viral RNA than the adults were.
Terrifying right? I mean, are kids just virus factories? Are they weapons of mass dissemination? Does 1000-times more viral RNA mean 1000 times more contagious? Or the question underneath all these questions – when schools open, will cases explode?
The study can’t tell us that. Note that I keep saying viral RNA, not virus. We do not know if these kids were shedding live virus that was actively capable of infecting others. The authors did not do viral cultures or other infectivity assays. So the errors in the headline? The word contagious. Higher viral load does not necessarily mean more contagious.
Also, remember that these were sick kids, mostly. These were kids who came to medical attention. Even if they are shedding transmissible virus, if only a small number of kids get sick enough to be in a study like this we might still dodge the bullet. Selection bias is a hell of a drug.
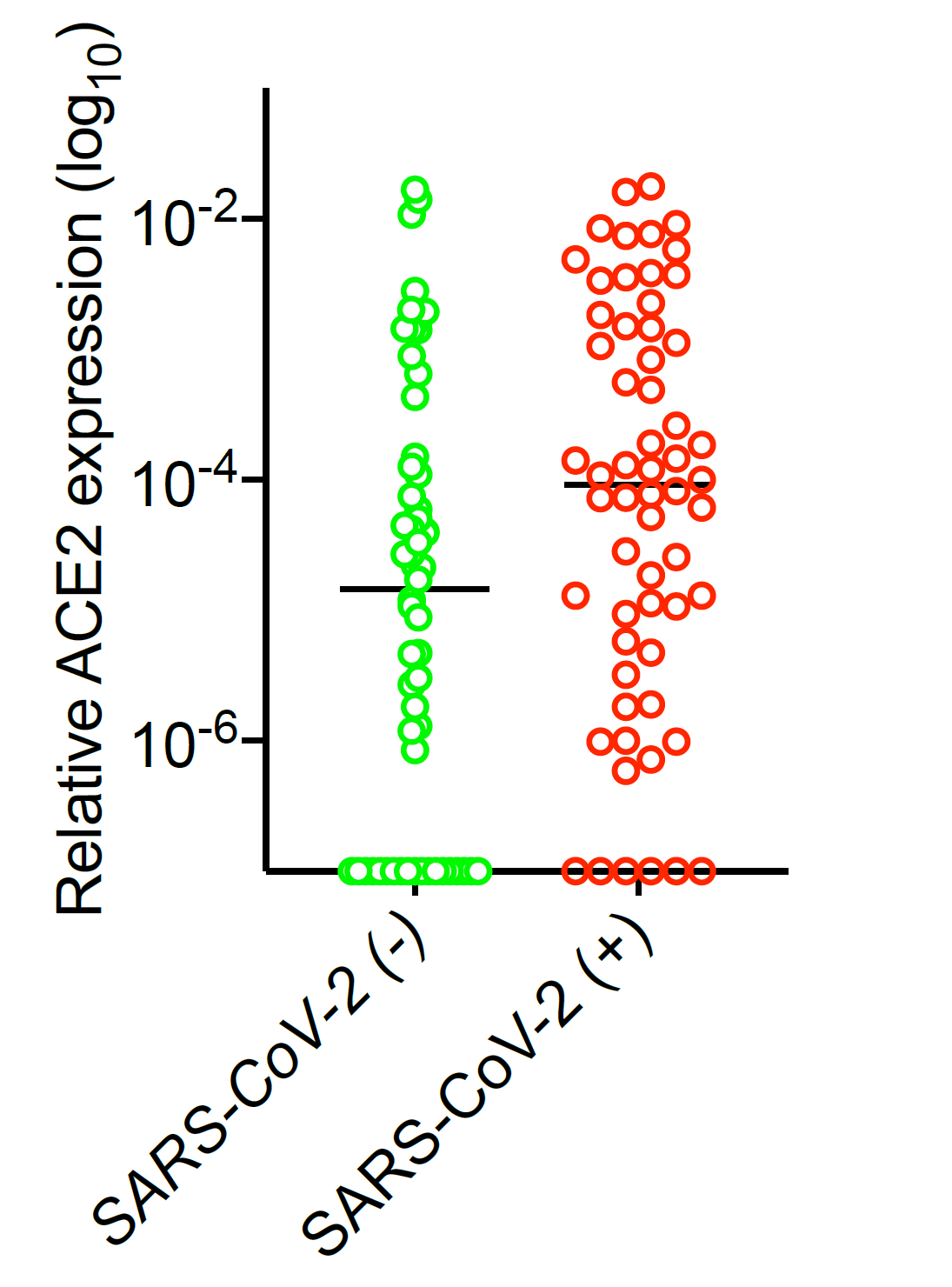
Kids who got infected had higher ACE-2 expression.
The study gives us a few other nuggets to digest as well. One big question is why kids don’t get a sick as adults when they contract COVID. You’ll remember that the receptor SARS-COV-2 binds to on epithelial cells is called ACE-2. One hypothesis is that kids have lower ACE-2 levels, which might limit the ability of the virus to replicate. This study pours some cold water on that hypothesis. The COVID+ kids did have higher ACE-2 expression than COVID-negative kids, suggesting that maybe having lower ACE-2 levels protects against infection.
But once infected? ACE-2 levels had nothing to do with viral load. Once it’s in, it’s in. This does not appear to be the explanation for why kids don’t get as sick as adults.

But, once infected, ACE-2 levels didn’t really correlate with viral load.
So… what have we learned? This study lends support to the idea that kids have a bit of a tougher time getting infected due to their lower ACE-2 levels. But once infected, it’s clear that the virus does quite well in their nasal passages, at least well enough to make a ton of its own RNA. We don’t know how that translates to contagiousness.
But I’ll admit this study makes me worried about schools reopening. We can hope that kids aren’t quite as easily infected. We can hope that if infected they aren’t as contagious as their viral loads would suggest. But that’s a lot of hope in a pandemic that eats hope for breakfast.
There’s a lot we still don’t know. But in a few months, we’ll find out.
This commentary first appeared on medscape.com